
The Essentials
🎧 Listen
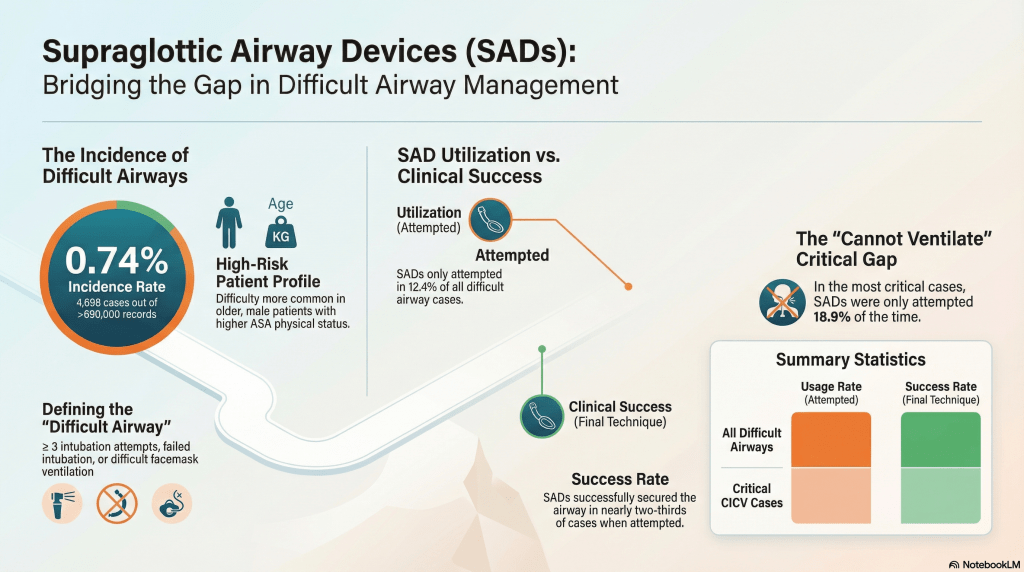
1️⃣ Difficult airway was uncommon — but real
- Among 658,104 general anaesthetics, difficult airway management occurred in 0.74% of cases.
- Most were triggered by:
- ≥ 3 intubation attempts (75%)
- Failed intubation (5%)
- Isolated difficult mask ventilation (20%)
Even in high-volume systems, true difficulty is rare — but when it happens, decisions matter.
2️⃣ Supraglottic airways were used less than guidelines suggest
- SADs were attempted in only 12.4% of difficult airway cases.
- This is striking given their prominent role in major difficult airway guidelines (e.g., DAS, Vortex).
Bottom line: SADs may be underutilized in real-world difficult airway management.
3️⃣ When used, success was moderate — not perfect
- Overall success rate of SAD in difficult airway cases: 65%
- In “cannot intubate, cannot facemask ventilate” situations:
- Used in 19% of cases
- Success rate: 63%
This is important. In real-world practice across all clinician experience levels, SAD success was not the >90% often quoted from smaller or specialist studies.
4️⃣ SAD was rarely attempted before surgical airway
- In the 22 cases that progressed to emergency front-of-neck airway:
- SAD was attempted in only one case
That finding raises critical questions about:
- Escalation behavior
- Guideline adherence
- Cognitive overload in crisis
- Whether a “best effort at all lifelines” approach is consistently applied
5️⃣ Prediction of difficulty was limited
- Only a small proportion of difficult airways were predicted pre-operatively.
- Even when both mask ventilation and intubation were anticipated to be difficult, SAD was infrequently planned as the primary device.
Planning and anticipation did not consistently translate into early SAD use.
6️⃣ Real-world data matters
This study represents:
- 75% of Danish anaesthesia departments
- All levels of clinician experience
- Everyday clinical practice, not simulation or expert airway teams
It reflects what actually happens — not what we think should happen.
Big Picture Implications
- SADs are foundational in difficult airway algorithms.
- Yet in practice, they are not frequently attempted.
- When used, they are moderately successful, not universally rescuing.
- There may be a gap between guideline design and human behavior under pressure.
This reinforces the importance of:
- Training for optimized SAD placement
- Explicit “best effort” attempts
- Cognitive tools that reduce hesitation and bias
- System-level reinforcement of structured escalation strategies
If you’d like, I can also:
- Convert this into a PAC-style infographic summary
- Frame it through the Vortex lens
- Or write a short interpretive commentary tying it to modern airway cognitive tools and human factors
🎧 Deep Cuts
The essentials give you the foundation.
This is where we sharpen it.
Time to be SAD? ABSOLUTELY!!
A LOOK AT THE EVIDENCE
Despite being around for years, supraglottic airway use remains sub-optimal in emergency or unexpectedly difficult airway scenarios. Don’t believe us? Review this study, then develop proficiency in supraglottic airway use to integrate them effectively into your practice.
What’s Next
Find Or Click Me
Nice work! To keep going, visit the next poster in our pop-up training space, or continue online by clicking the poster here.
Click below to return to the SGA menu.

Follow Us
You must be logged in to post a comment.