The First Supraglottic

Background
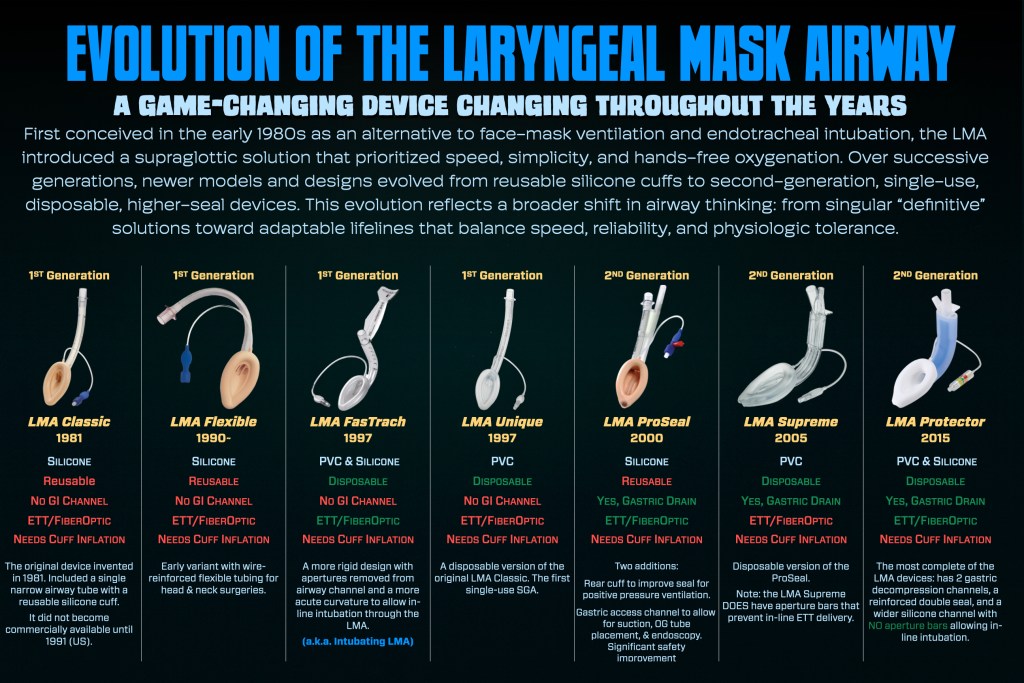
The laryngeal mask airway (LMA) was the first supraglottic device. It was discovered by Dr. Archibald Brain in 1981 as an alternative to FMV & ETT.
It is designed to sit over the laryngeal inlet and provide a hands-free conduit for oxygenation and ventilation without passing through the vocal cords. It occupies the middle ground between face-mask ventilation, basic airway adjuncts (OPA/NPA) and endotracheal intubation.
It is widely used in anesthesia, emergency airway management, and resuscitation as both a primary airway device and a rescue option when face mask ventilation or intubation is unsuccessful.
Here is a quick overview from ABCs of Anesthesia:
Description
The LMA Classic consists of:
- Airway tube: Connects to a bag-valve device or ventilator.
- Elliptical mask/cuff: Inflatable (in many models) and designed to seat over the glottic opening.
- Pilot balloon (inflatable types): Indicates cuff inflation status.
- 15 mm connector: Standard airway circuit connection.

Click Here to open a full-sized image in a new tab.
Modern generations of the LMA vary significantly and may include:
- Second-generation designs with gastric drainage channels
- Improved seal pressures
- Preformed or anatomically curved shafts
- Disposable and reusable options
- Wide, patent ventilation channels without bars to allow for inline ETT delivery,
Because performance characteristics vary, clinicians should be familiar with the specific device used in their institution.
Click Here to open a full-sized image in a new tab.
Second-generation LMAs with gastric access improve aspiration risk mitigation but do not eliminate it. Clinical judgment is essential.
Sizing
LMA size selection is generally based on patient weight (check manufacturer guidance). Typical adult ranges:
- Size 3: small adults (~30–50 kg)
- Size 4: average adults (~50–70 kg)
- Size 5: large adults (~70–100 kg)
- Size 6: very large adults (>100 kg)
Using too small a device results in poor seal and leak. Too large increases trauma risk and insertion difficulty.
Always confirm the specific sizing table for the device you are using.
🎧 Deep Cuts
The essentials give you the foundation.
This is where we sharpen it.
Here you’ll find high-impact clinical pearls, deeper analysis, and carefully curated learning resources that expand what matters most in real practice. Explore as much as you like. When you’re ready, step back into the essentials and continue the journey at the next poster.
Click Here for More
What’s Next
Find Or Click Me
Nice work! To keep going, visit the next poster in our pop-up training space, or continue online by clicking the poster here.
Click below to return to the SGA menu.
Follow Us
You must be logged in to post a comment.