
The Essentials
In airway management, there are tools you use—and then there are tools that define the outcome. The endotracheal tube is the latter. It’s the definitive airway: a direct, reliable conduit for oxygenation and ventilation, a seal against aspiration, and the final common pathway of resuscitation, anesthesia, and critical care.

Click Here to open the image in a new tab.
{kind=link}
The Definitive Airway
Why the ETT is the “Definitive Airway”
An endotracheal tube creates a controlled airway by:
- Bypassing the upper airway (tongue, edema, secretions, blood, obstruction).
- Securing the trachea to ensure consistent ventilation—even during transport, procedures, or CPR.
- Enabling positive-pressure ventilation and precise control of oxygenation/CO₂ clearance.
- Reducing aspiration risk by sealing the trachea with an inflatable cuff (when used appropriately).
- Providing a stable platform for suctioning, bronchoscopy, recruitment maneuvers, and advanced ventilator strategies.
Clinical Uses of the ETT
Uses: Where the ETT Lives in Clinical Practice
The ETT isn’t “one procedure.” It’s an infrastructure tool used across:
- Emergency medicine and prehospital care: definitive airway for respiratory failure, trauma, arrest.
- Anesthesia: controlled airway for surgery, paralysis, and mechanical ventilation.
- ICU and critical care: prolonged ventilation, lung-protective strategies, and bronchoscopy access.
- Procedural sedation rescue: when oxygenation/ventilation can’t be maintained non-invasively.
Endotracheal Tube Anatomy

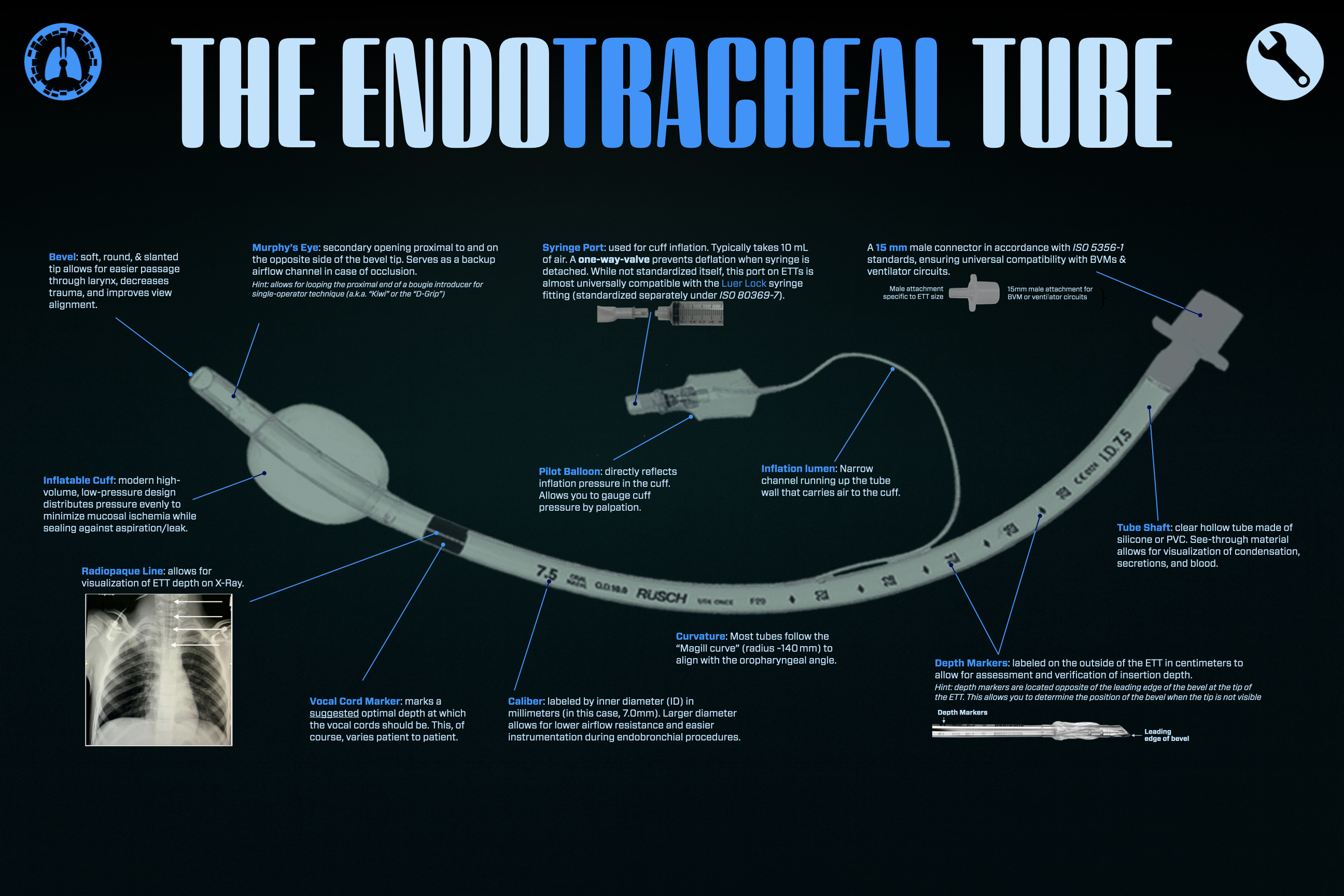
Anatomy of an ETT (Piece-by-Piece Breakdown)
1) 15 mm Connector (Machine End)
A universal interface that connects to a bag-valve-mask (BVM), ventilator circuit, or anesthesia circuit—built for fast compatibility when seconds count.
2) Tube Shaft (The Body)
The transparent cylindrical body is more than plastic:
- Inner diameter (ID) determines airflow resistance and ease of suction/bronchoscopy.
- Wall thickness/material influences rigidity, kink resistance, and cold-temperature behavior.
- Curvature (often a Magill-style curve) helps the tube follow the anatomy from the mouth to the trachea.
3) Depth Markings
Centimeter markings provide a quick visual reference for insertion depth and post-intubation migration—especially useful during transport or after repositioning.
4) Radiopaque Line
A built-in marker visible on X-ray that helps confirm tube position and track migration—critical when clinical signs are confusing or patient anatomy is challenging.
5) Distal Tip & Bevel
The beveled tip eases passage through the vocal cords and helps guide the tube along the tracheal axis. It’s the point of contact with delicate airway tissue—shape and smoothness matter.
6) The Murphy Eye
A small side opening near the tip that can preserve airflow if the main bevel becomes occluded against the tracheal wall or by secretions—one of the simplest, highest-impact safety features in airway design.
7) The Cuff (When Present)
The cuff forms a seal between the tube and tracheal wall to:
- minimize leak during ventilation,
- reduce aspiration risk,
- stabilize tube position.
Modern cuffs aim to seal at safe pressures—because too much pressure injures mucosa, and too little invites leak and microaspiration.
8) Inflation Lumen
A small channel running alongside the tube wall that carries air to the cuff.
9) Pilot Balloon + One-Way Valve
The pilot balloon reflects cuff inflation and provides the port for inflation/deflation. The one-way valve holds pressure to maintain a stable seal.
Variants: Different Tubes for Different Problems
Not all ETTs are the same—and choosing the right one matters.
Cuffed vs Uncuffed
- Cuffed: standard in most adults; better seal and ventilation control.
- Uncuffed: still used in select pediatric contexts and niche scenarios, depending on protocol and patient anatomy.
Reinforced (Armored) Tubes
Wire-reinforced construction resists kinking—useful when the head/neck position is extreme or the tube will be under compression.
RAE (Preformed) Tubes
Pre-shaped tubes designed to keep the circuit out of the surgical field—often used in ENT/dental cases.
Laser-Resistant Tubes
Designed for airway laser procedures, balancing safety with ventilation demands.
Subglottic Suction (SSD) Tubes
Add a suction port above the cuff to remove pooled secretions—an infection-prevention strategy in ventilated patients.
A Brief History: From Concept to Standard of Care
The ETT represents the evolution of airway control:
- Early airway instrumentation matured alongside the rise of direct laryngoscopy and surgical anesthesia.
- The 20th century saw refinement in curves, materials, and safety features—including the now-standard Murphy eye.
- The shift from reusable rubber to clear disposable plastics improved consistency, sterility, and visibility.
- Cuff technology evolved to support safer sealing and reduced mucosal injury.
Today’s ETT is the product of decades of iterative design—built for real-world use in blood, vomit, edema, trauma, time pressure, and physiologic collapse.
Deep Cuts
What are ETTs designed for? Is it tracheal access? Or Something Else?
The Bottom Line
The endotracheal tube is more than just a plastic conduit; it is the definitive tool for airway control. Every feature of the tube exists for a reason: oxygenation, ventilation, protection from aspiration, confirmation of placement, and safe long-term airway management. Understanding the anatomy of the ETT is fundamental to mastering airway management itself. Device fluency matters. When seconds count, clinicians who truly understand their tools perform with greater speed, precision, and confidence.
What’s Next
Nice work! To keep going, visit the next poster in our pop-up training space, or continue online by clicking the poster here.

You must be logged in to post a comment.