An Expert Guide On How to Decide
Overview
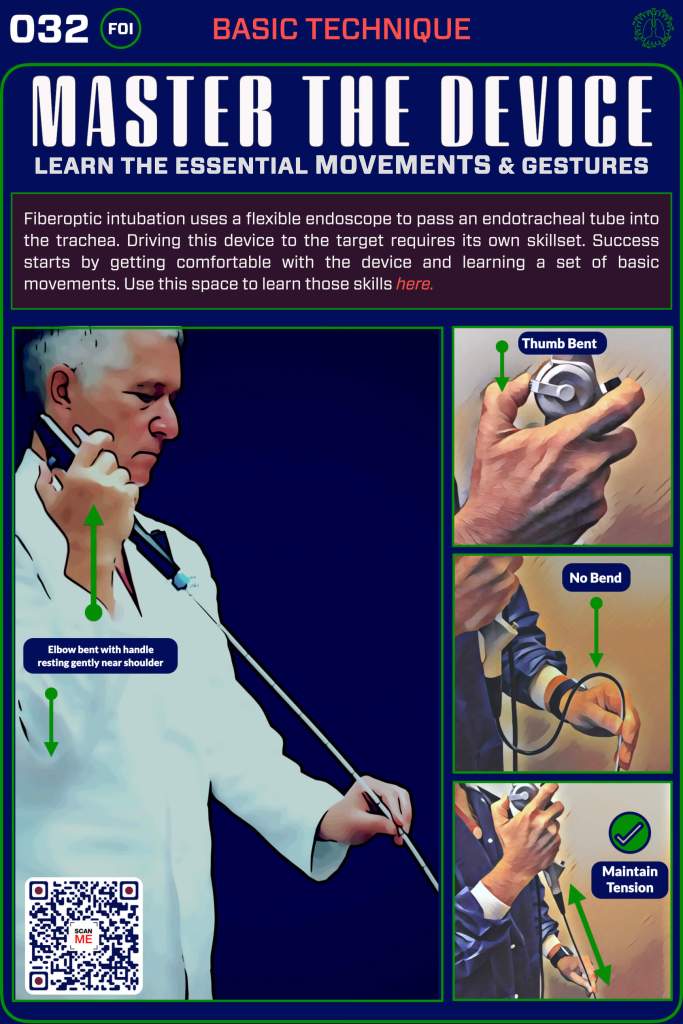
It seems counter-intuitive in the age of the video laryngoscope, but the fiberoptic approach to intubation is still considered the gold standard, even when the overwhelming majority of intubations today are performed with a laryngoscope. In spite of this, there are still specific situations in which a fiberoptic approach may be the best option. Here, we’ll spend some time getting to the bottom of that question, and give you a simple approach to help you decide if FOI is right in any clinical context.

When You Want Them Breathing
Fiberoptic intubation (FOI) is most relevant when you want to keep your patient breathing because you’re concerned that the use of a paralytic agent (most commonly with RSI) might have adverse consequences. If your patient has a known or predicted anatomically difficult airway and they are currently breathing on their own, the last thing you want to do is make the situation worse. This is where FOI shines because it can be performed “awake” using light sedation and topicalization (something we will show you how to do later), allowing you to preserve and protect a patient’s respiratory drive.
The patients where this applies are most commonly those with known or predicted anatomically difficult airways in which the use of RSI might create a failed airway and/or a can’t intubate, can’t oxygenate situation (CICO). Here are some of the clinical scenarios for which this concern might apply 👇
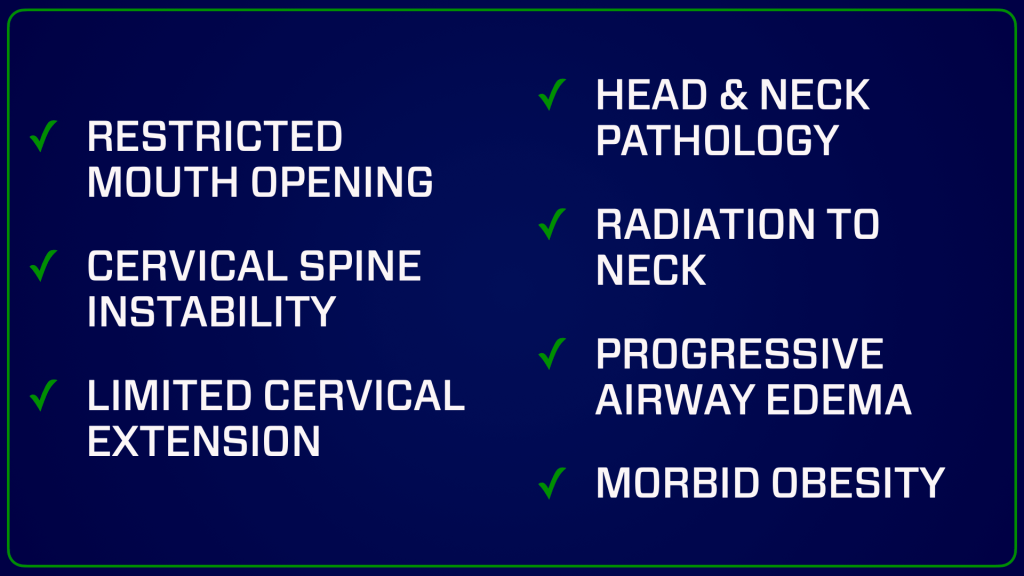
Indications for AFOI
As Rescue Tool
The Clinical Context
Certainly a consideration for the use of AFOI in the known or predicted difficult airway makes sense, particularly in the patient undergoing an elective procedure, but this is not the whole picture. What if your patient is in extremis or unstable. What then? Is AFOI still a good choice? The second biggest factor in deciding whether AFOI is right for your patient is: what are the conditions of the situation. In other words, what is the context.

AFOI takes more time than RSI and you need to have certain favorable conditions to tip the scales in favor of it. In general emergent situations that require multiple rapid interventions make FOI a less viable option. Here are some things to consider:

One Last Question
How good are you? No, seriously…
As clinicians we must always take our ego out of the equation. If you only rarely use a fiberoptic device, or have not practiced regularly to keep your skills up, you should reconsider the FOI approach. Either call for help, or if there is no other option, stick to the technique you are most comfortable with.
3 questions
Contraindications
What’s Next
Find Or Click Me
Nice work—you’re through this section! To keep going, scan the QR code on the physical poster at the next station in our pop-up training space to access the next set of digital content. Prefer to stay online? Just click the poster image here to continue your journey.