“A simple tool that turns obstruction into oxygenation.”

The Essentials
Overview
The oropharyngeal airway (OPA) is a rigid, curved adjunct designed to keep the upper airway patent by preventing posterior displacement of the tongue and soft tissues against the posterior pharyngeal wall. It is a basic, fast, low-cost intervention used to facilitate oxygenation and ventilation, most commonly during bag-mask ventilation (BMV) and resuscitation.
Description
An OPA is typically made of hard plastic and consists of:
- Flange (bite block): Rests on the lips/teeth and limits depth of insertion, can reduce occlusion from biting.
- Curved body: Conforms to oral and pharyngeal anatomy.
- Distal tip: Sits above the epiglottis in the oropharynx when properly positioned.
OPAs come in multiple sizes (often color-coded by manufacturer). Proper sizing and correct insertion technique determine success and reduce complications.
Indications
Use an OPA when you need airway patency in a patient who cannot reliably maintain their own airway.
Common indications:
- Unconscious patient with absent or markedly blunted gag reflex
- Airway obstruction from tongue/soft tissue collapse (snoring respirations, poor air entry with BMV)
- To facilitate effective BMV (improves seal and reduces obstruction)
- During resuscitation (CPR, peri-intubation optimization, post-intubation bite protection in select settings)
Clinical goal: improve alveolar ventilation/oxygen delivery by reducing upper airway obstruction.
Contraindications
Absolute (practical)
- Intact gag reflex / awake or semiawake patient
- High likelihood of gagging, vomiting, and laryngospasm.
Relative
- Significant oral trauma (unstable teeth, severe mucosal injury)
- Recent oral surgery or known friable oral tissues
- Severe trismus or inability to open the mouth adequately
- Ongoing active vomiting (risk of aspiration, consider alternative strategy)
If an OPA is not tolerated or triggers gagging, move to alternatives (positioning, jaw thrust, NPA if appropriate, two-person BMV optimization).
Sizing
Correct size matters. Too small can push the tongue backward or fail to relieve obstruction, too large can cause trauma or worsen obstruction.
Standard sizing method:
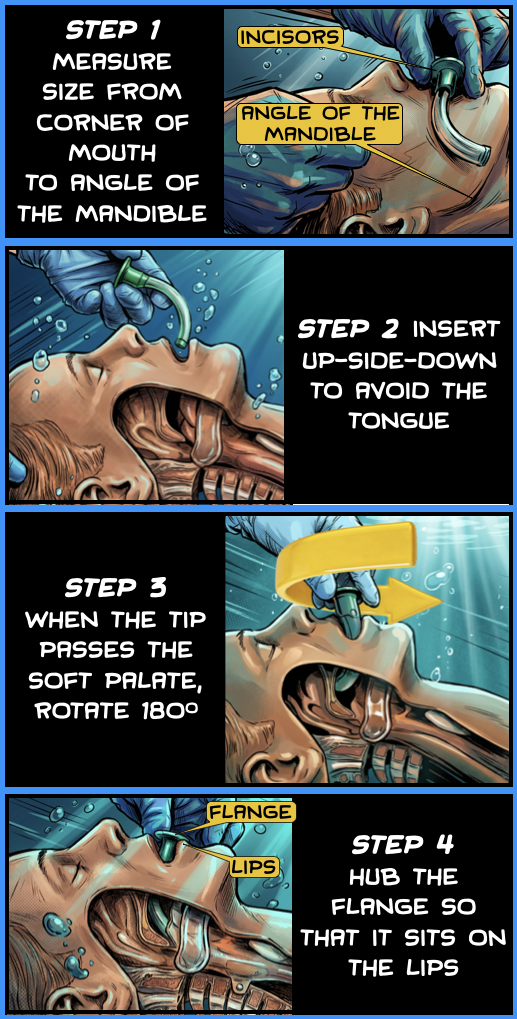
- Measure from the corner of the mouth to the angle of the mandible.
Quick clinical check:
- The flange should rest on the lips, and the distal tip should reach the oropharynx without “bottoming out” or riding shallow.

When in doubt between two sizes, it’s often safer to start with the size that matches the corner-of-mouth to angle-of-mandible measurement, then adjust based on effectiveness and tolerance.
Technique for Placement
Preparation
- Position: Place the patient in a sniffing or neutral position appropriate to context; use head tilt–chin lift or jaw thrust as needed (jaw thrust if trauma concerns).
- Suction: Clear blood, secretions, or vomitus as feasible.
Insertion (Adult)
Two common approaches are used; choose the one that minimizes trauma and maximizes control.
Method A: 180° rotation (classic adult technique)
- Open the mouth using a scissor technique or jaw thrust.
- Insert the OPA upside down (concavity facing up) along the tongue.
- Advance until the distal tip approaches the soft palate.
- Rotate 180° so the concavity faces down, following the curve of the tongue.
- Seat the flange on the lips/teeth.
Method B: Tongue depressor / direct insertion
- Use a tongue depressor (or laryngoscope blade if appropriate) to move the tongue forward.
- Insert the OPA in its final orientation (concavity down) without rotation.
- Advance gently until the flange rests on the lips.
Method B can reduce the risk of pushing the tongue posteriorly and may reduce mucosal injury in some hands, but it requires more deliberate control.
Confirmation of Effect
- Improved ease of BMV (less resistance, better chest rise)
- Reduced “snoring” or obstructive sounds
- Improved ventilation parameters if monitored (capnography waveform during BMV, oxygenation trends)
Troubleshooting and Removal
- Gagging/vomiting: remove immediately, suction, reposition, consider an alternative adjunct.
- Worsened obstruction: suspect incorrect size or malposition; remove and re-size, optimize head position and jaw thrust.
- Remove when the patient regains airway reflexes or can maintain their airway, unless it is serving a specific role under close monitoring.
Complications (worth knowing)
- Dental or soft tissue trauma, bleeding
- Gagging, vomiting, aspiration
- Laryngospasm (especially if not deeply unconscious)
- Worsened obstruction from incorrect sizing or placement
🎧 Deep Cuts
The essentials give you the foundation.
This is where we sharpen it.
Click Here for More
This longer video demonstrates how to insert an oropharyngeal airway (OPA) by the great educators at GeekyMedics. Another great resource to add to your learning network. It’s worth the watch.
What’s Next
Find Or Click Me
Nice work! To keep going, visit the next poster in our pop-up training space, or continue online by clicking the poster here.
Click below to return to the FMV menu.
Follow Us
You must be logged in to post a comment.