NextGen Learning To Elevate Your Airway Practice
Start Here
The Value of POCUS
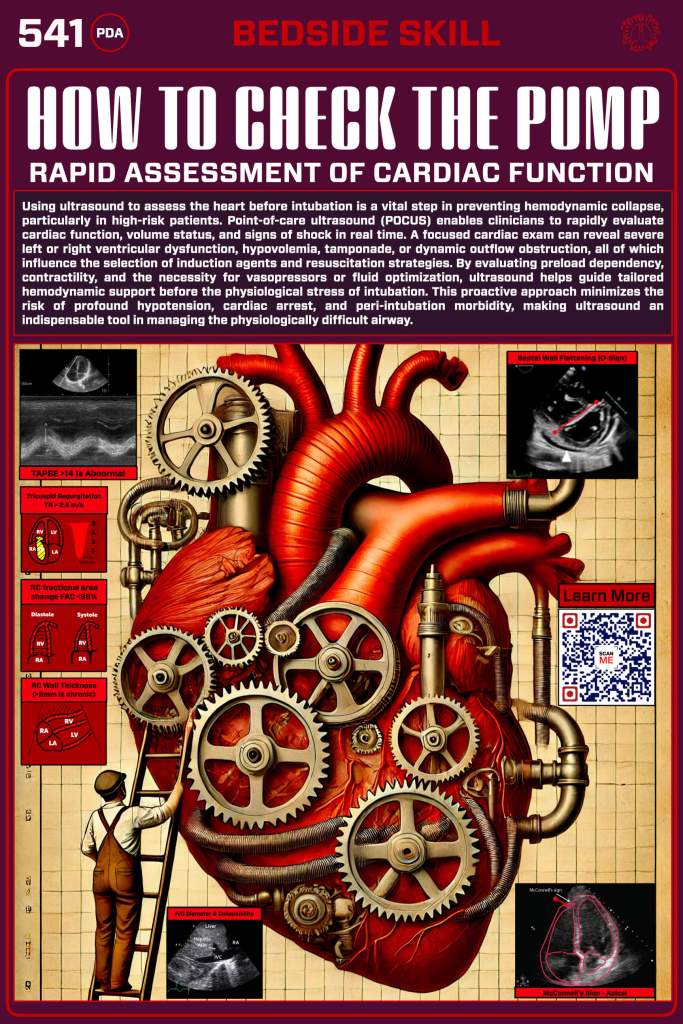
Using ultrasound to assess the heart prior to intubation is a critical step in preventing hemodynamic collapse, especially in high-risk patients. Point-of-care ultrasound (POCUS) allows clinicians to rapidly evaluate cardiac function, volume status, and signs of shock in real-time. A focused POCUS cardiac exam can identify severe left or right ventricular dysfunction, hypovolemia, tamponade, or dynamic outflow obstruction, all of which influence the choice of induction agents and resuscitative strategies. It’s time to learn how to do it.
Contractility: Is the Heart Squeezing?
Ultrasound gives you an instant look at global contractility, telling you whether the heart is pumping effectively or barely moving at all. With just a parasternal long-axis (PLAX), apical four-chamber (A4C), or subxiphoid view, you can quickly assess how well the ventricles are squeezing, if the ejection fraction looks decent or if you’re dealing with a weak, failing heart that won’t tolerate the next step. If the walls are barely moving, stroke volume is crashing, and the ventricle looks like it’s taking a nap—you know this patient needs hemodynamic support before you push induction meds.
the Apical 4 Chamber View
The best way to evaluate RV contractility is to get a good apical four-chamber view. Is the RV bigger than the LV? That’s a sign of RV dysfunction.
Is There Enough Volume? How to Assess Preload
In a critically ill patient, preload determines whether the heart has enough blood to pump forward or if it’s running on empty. But how do you know if your patient is fluid-responsive or on the edge of volume overload? Ultrasound gives you the answer in seconds. A quick look at the inferior vena cava (IVC) tells you if the tank is full or depleted—a collapsing IVC suggests low preload, while a fat, non-collapsing IVC may mean fluid won’t help or could even make things worse. Need more confirmation? Look for a hyperdynamic left ventricle in a patient screaming for fluids or a dilated, strained right heart where fluid could be dangerous.
Assessing Volume Status
A plethoric IVC suggests a volume overload state or obstructive pathology (tamponade, PE). >50% collapse with inspiration or compression suggests euvolemia or hypovolemia. The RV is preload dependent to an extent, but excess fluid can quickly overload the RV and worsen RV dysfunction–so consider vasopressors early.
Too Much Back Pressure? How to Assess Venous Congestion
When a critically ill patient is deteriorating, venous congestion is the silent killer—it chokes organ perfusion, worsens shock, and makes fluid management a dangerous guessing game. But ultrasound can show you the warning signs before it’s too late. A plump, non-collapsing IVC suggests high right-sided pressures, but the real game-changer is the Doppler assessment of the hepatic, portal, and renal veins. A pulsatile portal vein? A discontinuous, reversed renal vein Doppler? These are red flags for systemic venous congestion, signaling that more fluids could push the patient into worsening organ dysfunction. If the right heart is failing and pressure is backing up into the venous system, diuresis or inotropes—not more fluids—might be the key —because what’s behind the heart matters just as much as what’s in front of it.
The VEXUS Score: A Systematic Approach to Assessing Venous Congestion
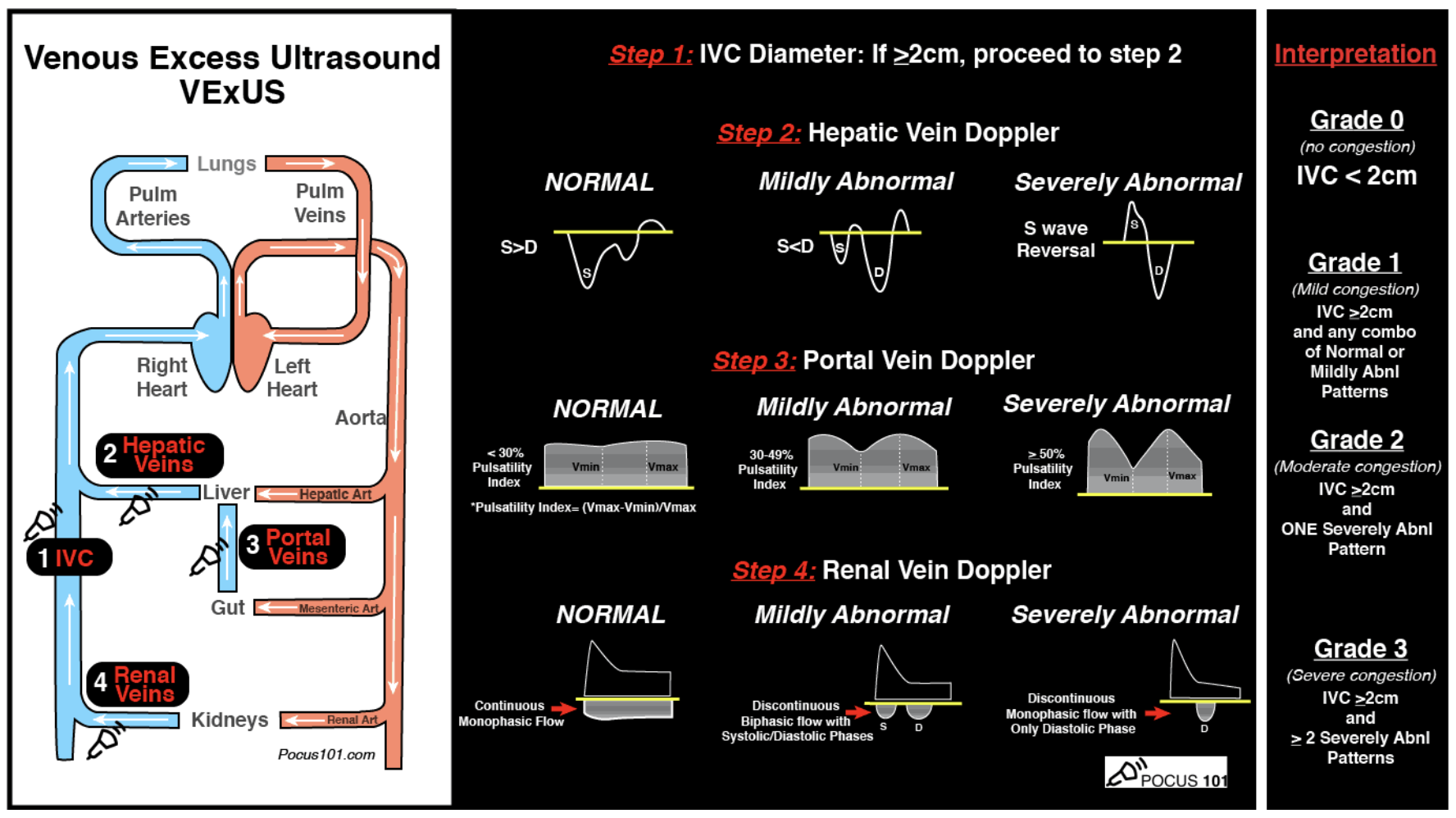
The VEXUS (Venous Excess) Score is a bedside ultrasound tool that helps identify systemic venous congestion and its impact on organ perfusion. It combines assessments of the IVC, hepatic vein, portal vein, and renal vein Doppler waveforms to determine the severity of venous congestion.
- IVC Size & Collapsibility: A dilated, non-collapsing IVC suggests high right atrial pressure.
- Hepatic Vein Doppler: Normal flow is triphasic, but congestion leads to blunted or reversed flow.
- Portal Vein Doppler: Normally continuous; pulsatility indicates worsening congestion.
- Renal Vein Doppler: Normal flow is continuous, but congestion causes pulsatility or even flow reversal, signaling kidney dysfunction.
The VEXUS score helps distinguish fluid-responsive patients from those at risk for volume overload and organ congestion, guiding resuscitation decisions in critically ill patients. Instead of guessing, VEXUS lets you see if fluids will help—or hurt.
Is the Right Heart Struggling? How to Use Ultrasound to Assess RV Dysfunction
The right ventricle (RV) is fragile. Unlike the left ventricle, it is thin-walled and pressure-sensitive, meaning volume overload, pulmonary hypertension, or increased afterload can push it into failure. The good news? Ultrasound gives you the answer in seconds.
Here’s what to look for:
- RV Size: A dilated RV (RV: LV ratio >0.6 on PLAX or >1:1 on A4C) is a red flag for strain.
- Septal Flattening (“D Sign”) on the parasternal short axis (PSAX) suggests RV pressure overload (think PE or severe pulmonary hypertension).
- TAPSE (Tricuspid Annular Plane Systolic Excursion) <16mm or S’ wave <9.5 cm/s on Tissue Doppler means the RV isn’t contracting well.
- McConnell’s Sign – A hyperkinetic RV apex with a weak free wall? Think massive PE until proven otherwise.
- IVC Engorgement with minimal collapse suggests RV failure with venous congestion.
If you see a dilated, poorly contracting RV, this patient won’t tolerate positive pressure ventilation without major hemodynamic support. Before you intubate, optimize preload, avoid hypoxia/hypercapnia, and be ready with pressors or inotropes. The RV is the weak link in many critically ill patients—find it before it fails.
TAPSE: Is it Acute or Chronic?
Tricuspid annular plane systolic excursion (TAPSE) has a strange name but is simple to measure. It’s done in the apical 4-chamber view using m-mode. We show you how to do it here. Is the measurement less than 1.6cm? That means poor contractility.
The Bottom Line
Point-of-care ultrasound (POCUS) can provide critical real-time insights using a few key views to assess cardiac function rapidly before intubation. The parasternal long-axis (PLAX) view clearly examines left ventricular function and overall contractility. The apical four-chamber (A4C) view helps evaluate both ventricles, chamber sizes, and signs of right heart strain. The subxiphoid (subcostal) view is a great alternative when transthoracic windows are poor, offering a broad look at global cardiac activity. Finally, the inferior vena cava (IVC) view assesses volume status and preload sensitivity by evaluating collapsibility. These focused ultrasound views allow clinicians to quickly identify severe dysfunction, tamponade, hypovolemia, or right heart strain, helping guide resuscitation and optimize hemodynamics before airway management. Fast, focused, and lifesaving—ultrasound is a game-changer for high-risk intubations.
What’s Next
Find Or Click Me
Nice work—you’re through this section! To keep going, scan the QR code on the physical poster at the next station in our pop-up training space to access the next set of digital content. Prefer to stay online? Just click the poster image here to continue your journey.

You must be logged in to post a comment.