NextGen Learning To Elevate Your Airway Practice
Start Here
The Essentials
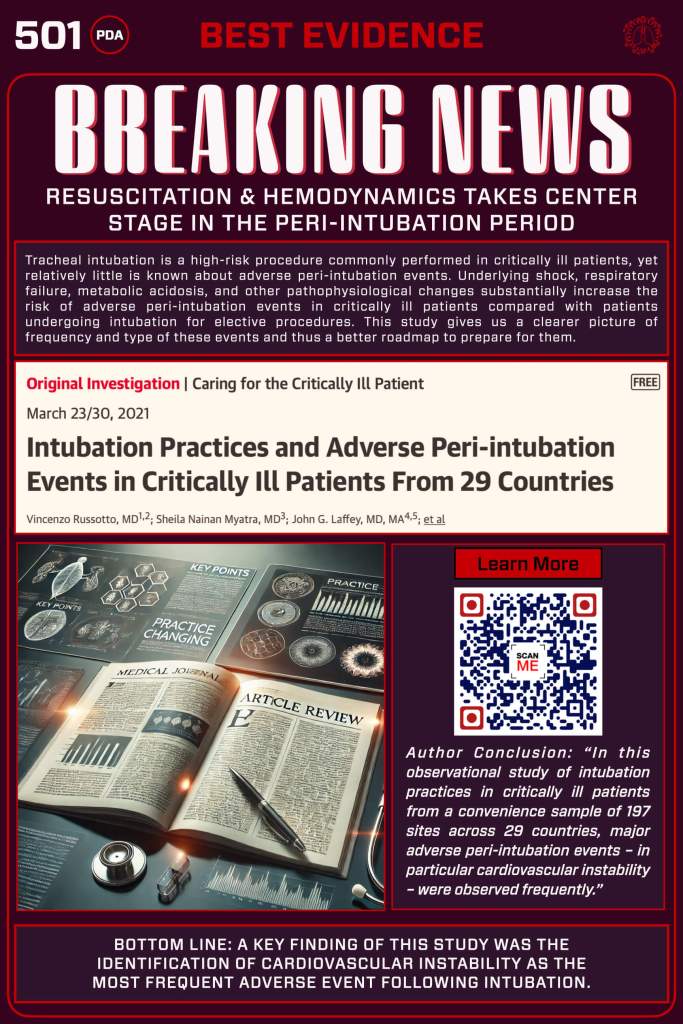
How the INTUBE Study Changed the Game
Not too long ago, the focus of airway management was primarily on anatomy — can you see the cords, can you pass the tube. But the INTUBE study shattered that narrow lens by pulling global data from 29 countries and putting numbers to a reality frontline clinicians have always known: the greatest danger during intubation isn’t just a difficult laryngoscopy — it’s the crashing physiology.
With nearly half of critically ill patients experiencing major peri-intubation events like cardiovascular collapse, hypoxemia, or cardiac arrest, the study reframed the conversation. It’s not just about passing the tube; it’s about preparing the patient. The INTUBE data elevated the concept of the physiologically difficult airway from a niche discussion to a global call for better preoxygenation, hemodynamic preparation, sedative choice, and resuscitative planning.
This landmark work doesn’t just highlight bad outcomes — it challenges us to rethink what “difficult airway” really means and pushes airway clinicians everywhere to transform practice, so we resuscitate before we intubate.
🎧 Deep Cuts
You’ve got the basics down—great work! To keep learning, you can take a deep dive on this material, or head to the next poster. Oh, you want to go deeper? Click Below for extra clinical pearls, evidence reviews, and curated links to expand your learning network—or bookmark it and return anytime.
Click Here for a Deeper Dive on this Study
🎸 Great! Welcome to the Deeper Cuts for this Topic
Study Overview
- Objective: To evaluate the incidence and nature of major adverse peri-intubation events and assess current intubation practices in critically ill patients.
- Primary Outcome: Incidence of major adverse peri-intubation events within 30 minutes of intubation, defined as:
- Cardiovascular instability (e.g., systolic blood pressure <65 mm Hg at least once, <90 mm Hg for >30 minutes, new or increased need for vasopressors, or fluid bolus >15 mL/kg)
- Severe hypoxemia (peripheral oxygen saturation <80%)
- Cardiac arrest
- Secondary Outcomes: Intensive care unit (ICU) mortality and other complications such as esophageal intubation, arrhythmias, aspiration, and pneumothorax.ResearchGate+1Wikipedia+1
Key Findings
- Major Adverse Events: 45.2% of patients experienced at least one major adverse peri-intubation event.
- Cardiovascular Instability: The most common event, occurring in 42.6% of patients.
- Severe Hypoxemia: Occurred in 9.3% of patients.
- Cardiac Arrest: Reported in 3.1% of cases, with a 52.7% return of spontaneous circulation rate.
- ICU Mortality: Overall rate was 32.8%; notably, patients who experienced major adverse events had a higher mortality rate (40.7%) compared to those who did not (26.3%).
Intubation Practices Observed
- Preoxygenation Methods:
- Bag-valve mask: 62.4%
- Standard face mask: 13.2%
- Non-invasive ventilation: 11.6%
- High-flow nasal cannula: 5.4%
- Apneic Oxygenation: Utilized in 10.4% of cases.
- Rapid Sequence Induction (RSI): Employed in 62.2% of intubations.
- Induction Agents:
- Propofol: 41.5%
- Midazolam: 36.4%
- Etomidate: 17.8%
- Ketamine: 14.2%
- Neuromuscular Blockers:
- Rocuronium: 41.8%
- Succinylcholine: 21.8%
- Laryngoscopy Techniques:
- Direct laryngoscopy: 81.5%
- Video laryngoscopy: 17.1%
- First-Pass Success Rate: Achieved in 79.8% of intubations.
- Confirmation of Intubation:
- Auscultation: 57.9%
- Waveform capnography: 25.6%
- Notably, capnography was not used in 68.9% of esophageal intubation cases.
Clinical Implications
The INTUBE study highlights the high incidence of major adverse events, particularly cardiovascular instability, during tracheal intubation in critically ill patients. These findings underscore the importance of:
- Pre-intubation Optimization: Implementing strategies such as fluid resuscitation and vasopressor support to stabilize hemodynamics before intubation.
- Sedative Selection: Considering the hemodynamic effects of induction agents; for instance, propofol was associated with higher rates of cardiovascular instability compared to etomidate.
- Use of Capnography: Enhancing the use of waveform capnography to confirm endotracheal tube placement and reduce the risk of unrecognized esophageal intubation.
- First-Pass Success: Striving for first-attempt intubation success to minimize the risk of complications.
Limitations
- Study Design: As an observational study, it cannot establish causality between intubation practices and adverse events.
- Data Collection: Potential for self-reporting bias and underreporting of adverse events.
- Sample Selection: Use of a convenience sample may limit the generalizability of findings.
- Lack of Granular Data: Limited information on specific interventions used to mitigate adverse events and on long-term patient outcomes.
Conclusion
The INTUBE study provides valuable insights into the risks associated with tracheal intubation in critically ill patients, emphasizing the need for careful preparation and adherence to best practices to minimize adverse events. Clinicians should focus on hemodynamic optimization, appropriate sedative selection, and the use of capnography to improve patient outcomes during intubation.
For a more detailed analysis and discussion of the INTUBE study, you may refer to the full article published in JAMA: JAMA Network
Curated MedEd
Check out this great review by REBEL EM and then add them to your learning network!
The Bottom Line
The INTUBE and other more recent studies like the BARCO study out of Brazil shows that in critically ill patients, the biggest threats during intubation come not from anatomy but from unstable physiology — nearly half experience major adverse events like hypotension, hypoxemia, or cardiac arrest. Managing the physiologically difficult airway means optimizing the patient before you push drugs or pass the tube. Prepare, resuscitate, and plan — because the tube won’t fix a failing system.
New Section
What’s Next
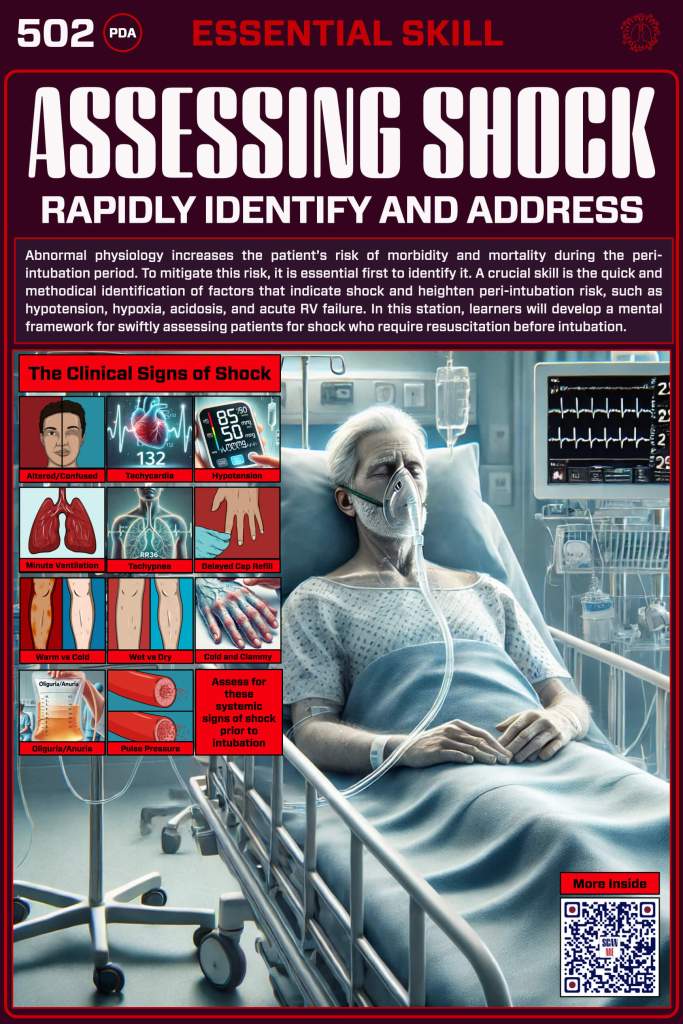
You can’t effectively resuscitate in the peri-intubation period if you can’t identify shock physiology and its underlying impact on key organ systems such as the lungs, the vasculature, and the heart. The following section is all about performing a rapid assessment before intubation to guide your resuscitation.
Find Or Click Me
Nice work—you’re through this section! To keep going, scan the QR code on the physical poster at the next station in our pop-up training space to access the next set of digital content. Prefer to stay online? Just click the poster image here to continue your journey.
You must be logged in to post a comment.