Leverage the Full Potential of These Devices
The Essentials
What Every Clinician Should Know Before Using a Video Laryngoscope
Video laryngoscopy expands your options, but it also demands a clear understanding of the device in your hands. Before you pick up a video laryngoscope, there are a small number of essential concepts you must understand and a few predictable problems you should expect to encounter. This section focuses only on those differences and fundamentals. The goal is readiness: to help you succeed with video laryngoscopy before you ever place the device in a patient’s mouth.
🎧 Deep Cuts
You’ve covered the essentials, solid work. From here, you can move on to the next poster or tap on any of these topics to explore them in greater depth.
The History of Video Laryngoscopy
From Mirrors to Monitors: A History of VL
Video laryngoscopy has revolutionized airway management — not just by making intubation safer, but by unlocking entirely new ways to approach the airway. But this game-changing technology didn’t just materialize out of thin air. It’s the product of decades of innovation, trial and error, and bold thinking that pushed the boundaries of what’s possible. To understand where we’re headed, it helps to know where we’ve been. Take a moment to explore the history of VL — and see how we got from mirrors to monitors.

The History and Rise of Video Laryngoscopy
Airway management has always been a cornerstone of critical care, but for over a century, it has been a game of alignment, line of sight, and practiced hands. Direct laryngoscopy (DL), introduced by Chevalier Jackson in the early 1900s, revolutionized the field with rigid blades and illuminated views [1]. The technique relied on anatomical alignment, in which the oral, pharyngeal, and laryngeal axes were aligned to expose the vocal cords. It was a powerful tool — but one with limits.
Unlike direct laryngoscopy, video laryngoscopy decouples the view from the operator’s eye, projecting it onto a screen for visualization. This allowed for better visualization of the glottis, especially in cases with difficult anatomy or trauma, and enabled shared visualization, transforming intubation into a teachable, team-based event [4].
The First Glimpse: Origins of the Video Laryngoscope
The first true video laryngoscope was developed in the early 2000s, with the introduction of the GlideScope®, created by Canadian anesthesiologist Dr. John Pacey. It was approved by Health Canada in 2001 and later by the FDA in 2003 [2,3]. Inspired by a difficult intubation with spinal precautions, Pacey’s design featured a hyperangulated blade with a camera that transmitted a real-time image to a monitor. This concept radically changed how airway structures were visualized.
Evolution and Expansion: From Backup Tool to First-Line Standard
At first, video laryngoscopes were bulky, expensive, and often complicated to set up. As a result, they were mostly reserved for planned difficult airways or used as a backup after failed direct attempts. But over time, as designs became more user-friendly and the evidence grew in their favor, video laryngoscopy began to gain ground — not just as a rescue tool, but as a first-line option:
- A 2007 study showed VL significantly improved the Cormack-Lehane view compared to DL [5].
- Subsequent trials and meta-analyses have confirmed higher first-pass success rates and lower rates of esophageal intubation, especially in patients with difficult airways [6,7].
- In trauma and spine injury, VL showed reduced cervical spine movement during intubation [8].
Meanwhile, manufacturers such as Karl Storz, McGrath, and Verathon expanded the market with devices offering both Macintosh-style and hyperangulated blades, enabling flexible use across various clinical scenarios [9].
The first handheld video laryngoscope was developed in 2004 by a Scottish medical student named Matt McGrath. His creation (the epnonymous McGrath Series 5) was compact, battery-powered, and entirely self-contained, bringing video laryngoscopy out of the OR and into a more accessible, portable form. It marked a major leap forward, making handheld VL a viable option for routine use and expanding its reach beyond the operating room.
Perhaps most importantly, VL became a revolutionary educational tool. With real-time video, instructors can guide learners through complex airways without having to guess what the operator is seeing [10].
The COVID-19 pandemic further accelerated the shift: VL reduced provider exposure, enabled physical distancing, and became the default intubation method in many hospitals [11].
By the late 2010s, major guidelines such as the Difficult Airway Society (DAS) 2015 guidelines [12] and the ASA 2022 Practice Guidelines [13] began to recommend VL early in the algorithm, particularly in anticipated or encountered difficulty.
Current Trends: Ubiquity and Customization
Today, VL is integrated into the standard of care across emergency, ICU, anesthesia, and pre-hospital settings. Trends shaping its current use include:
- Handheld, wireless devices (e.g., GlideScope Go™, C-MAC Pocket Monitor) offer portability and are ideal for critical care and EMS [14].
- Hybrid approach: Many providers train on both VL and DL, but increasingly use VL as the first-line device for most intubations [15].
- Increased focus on delivery mechanics: As visualization becomes routine, attention has turned to tube delivery, stylet shaping, and operator positioning, particularly with hyperangulated blades [16].
The Future: Smarter, Smaller, and More Integrated
Looking forward, several trends are likely to define the next phase of VL evolution:
- AI-assisted laryngoscopy: Early prototypes show promise in real-time structure identification and view optimization, potentially guiding novice users through intubation steps [17].
- Augmented Reality (AR): Pilot studies are exploring overlays to aid training and procedural decision-making [18].
- Global access: Low-cost, disposable VL options may democratize airway management in low-resource and field environments [19].
- Simulation & remote coaching: Integrated recording and remote streaming capabilities are turning VL into a platform for telementoring and asynchronous feedback.
At the same time, there is growing concern about DL skill decay, particularly among new learners who are trained almost exclusively on VL [20]. Many programs are re-emphasizing progressive laryngoscopy techniques that work across device platforms to retain foundational skills.
Bottom Line
Video laryngoscopy didn’t just add a screen to a scope — it transformed the cognitive and technical framework of intubation. From a rescue tool to the frontline standard, VL has redefined how we teach, learn, and perform airway management. As technology continues to evolve, video laryngoscopy will remain a central — and increasingly intelligent — part of the clinician’s airway toolkit.
References
- Jackson C. The tracheotomy. The Laryngoscope. 1909;19(1):285–90.
- Pacey JA. GlideScope® Video Laryngoscope: A New Tool for Difficult Airways. Anesthesiology News. 2002.
- Verathon Inc. History of GlideScope. Accessed 2025.
- Sakles JC, et al. The Importance of Video Laryngoscopy as a Teaching Tool. Acad Emerg Med. 2012;19(7):857–8.
- Aziz MF, et al. Comparative effectiveness of the C-MAC video laryngoscope vs direct laryngoscopy. Anesthesiology. 2012;116(3):629–36.
- Lewis SR, et al. Video laryngoscopy vs direct laryngoscopy for adult tracheal intubation. Cochrane Database Syst Rev. 2016;(11): CD011136.
- Silverberg MJ, et al. Comparison of video and direct laryngoscopy in critically ill patients. Crit Care Med.2015;43(3):636–41.
- Turkstra TP, et al. Cervical spine motion: a comparison of video vs direct laryngoscopy. Anesthesiology. 2005;103(3):491–7.
- Doyle DJ. Videolaryngoscopy in the 21st century. Cleveland Clinic Journal of Medicine. 2021;88(5):263–4.
- Howard-Quijano K, et al. Video vs direct laryngoscopy teaching effectiveness. Anesth Analg. 2008;106(6):1651–4.
- Matava CT, et al. Safe Airway Management during COVID-19. Anesth Analg. 2020;131(1):61–73.
- Difficult Airway Society (DAS). Guidelines for the Management of Unanticipated Difficult Intubation in Adults. Br J Anaesth. 2015;115(6):827–48.
- American Society of Anesthesiologists (ASA). Practice Guidelines for Management of the Difficult Airway. Anesthesiology. 2022;136(1):31–81.
- Park L, et al. Use of handheld video laryngoscopes in the ICU. J Intensive Care Med. 2021;36(1):78–84.
- Sakles JC, et al. First-pass success rates with video vs direct laryngoscopy. Acad Emerg Med. 2013;20(7):617–23.
- Driver BE, et al. Optimizing Stylet Shaping for Hyperangulated Video Laryngoscopy. Ann Emerg Med. 2020;75(4):454–61.
- Yan Y, et al. Development of an AI system for airway structure identification in VL. J Biomed Inform. 2021;115:103704.
- Choi J, et al. Augmented reality in airway management training. J Clin Anesth. 2023;86:111086.
- Schricker T, et al. Disposable video laryngoscopes in austere environments. Can J Anesth. 2022;69(4):530–7.
- Kennedy CC, et al. Skill retention in direct laryngoscopy: a fading art? Chest. 2014;146(4):1189–95.
The History and Rise of Video Laryngoscopy
Airway management has always been a cornerstone of critical care, but for over a century, it has been a game of alignment, line of sight, and practiced hands. Direct laryngoscopy (DL), introduced by Chevalier Jackson in the early 1900s, revolutionized the field with rigid blades and illuminated views [1]. The technique relied on anatomical alignment, in which the oral, pharyngeal, and laryngeal axes were aligned to expose the vocal cords. It was a powerful tool — but one with limits.
Unlike direct laryngoscopy, video laryngoscopy decouples the view from the operator’s eye, projecting it onto a screen for visualization. This allowed for better visualization of the glottis, especially in cases with difficult anatomy or trauma, and enabled shared visualization, transforming intubation into a teachable, team-based event [4].
The First Glimpse: Origins of the Video Laryngoscope
The first true video laryngoscope was developed in the early 2000s, with the introduction of the GlideScope®, created by Canadian anesthesiologist Dr. John Pacey. It was approved by Health Canada in 2001 and later by the FDA in 2003 [2,3]. Inspired by a difficult intubation with spinal precautions, Pacey’s design featured a hyperangulated blade with a camera that transmitted a real-time image to a monitor. This concept radically changed how airway structures were visualized.
Evolution and Expansion: From Backup Tool to First-Line Standard
At first, video laryngoscopes were bulky, expensive, and often complicated to set up. As a result, they were mostly reserved for planned difficult airways or used as a backup after failed direct attempts. But over time, as designs became more user-friendly and the evidence grew in their favor, video laryngoscopy began to gain ground — not just as a rescue tool, but as a first-line option:
- A 2007 study showed VL significantly improved the Cormack-Lehane view compared to DL [5].
- Subsequent trials and meta-analyses have confirmed higher first-pass success rates and lower rates of esophageal intubation, especially in patients with difficult airways [6,7].
- In trauma and spine injury, VL showed reduced cervical spine movement during intubation [8].
Meanwhile, manufacturers such as Karl Storz, McGrath, and Verathon expanded the market with devices offering both Macintosh-style and hyperangulated blades, enabling flexible use across various clinical scenarios [9].
The first handheld video laryngoscope was developed in 2004 by a Scottish medical student named Matt McGrath. His creation (the epnonymous McGrath Series 5) was compact, battery-powered, and entirely self-contained, bringing video laryngoscopy out of the OR and into a more accessible, portable form. It marked a major leap forward, making handheld VL a viable option for routine use and expanding its reach beyond the operating room.
Perhaps most importantly, VL became a revolutionary educational tool. With real-time video, instructors can guide learners through complex airways without having to guess what the operator is seeing [10].
The COVID-19 pandemic further accelerated the shift: VL reduced provider exposure, enabled physical distancing, and became the default intubation method in many hospitals [11].
By the late 2010s, major guidelines such as the Difficult Airway Society (DAS) 2015 guidelines [12] and the ASA 2022 Practice Guidelines [13] began to recommend VL early in the algorithm, particularly in anticipated or encountered difficulty.
Current Trends: Ubiquity and Customization
Today, VL is integrated into the standard of care across emergency, ICU, anesthesia, and pre-hospital settings. Trends shaping its current use include:
- Handheld, wireless devices (e.g., GlideScope Go™, C-MAC Pocket Monitor) offer portability and are ideal for critical care and EMS [14].
- Hybrid approach: Many providers train on both VL and DL, but increasingly use VL as the first-line device for most intubations [15].
- Increased focus on delivery mechanics: As visualization becomes routine, attention has turned to tube delivery, stylet shaping, and operator positioning, particularly with hyperangulated blades [16].
The Future: Smarter, Smaller, and More Integrated
Looking forward, several trends are likely to define the next phase of VL evolution:
- AI-assisted laryngoscopy: Early prototypes show promise in real-time structure identification and view optimization, potentially guiding novice users through intubation steps [17].
- Augmented Reality (AR): Pilot studies are exploring overlays to aid training and procedural decision-making [18].
- Global access: Low-cost, disposable VL options may democratize airway management in low-resource and field environments [19].
- Simulation & remote coaching: Integrated recording and remote streaming capabilities are turning VL into a platform for telementoring and asynchronous feedback.
At the same time, there is growing concern about DL skill decay, particularly among new learners who are trained almost exclusively on VL [20]. Many programs are re-emphasizing progressive laryngoscopy techniques that work across device platforms to retain foundational skills.
Bottom Line
Video laryngoscopy didn’t just add a screen to a scope — it transformed the cognitive and technical framework of intubation. From a rescue tool to the frontline standard, VL has redefined how we teach, learn, and perform airway management. As technology continues to evolve, video laryngoscopy will remain a central — and increasingly intelligent — part of the clinician’s airway toolkit.
References
- Jackson C. The tracheotomy. The Laryngoscope. 1909;19(1):285–90.
- Pacey JA. GlideScope® Video Laryngoscope: A New Tool for Difficult Airways. Anesthesiology News. 2002.
- Verathon Inc. History of GlideScope. Accessed 2025.
- Sakles JC, et al. The Importance of Video Laryngoscopy as a Teaching Tool. Acad Emerg Med. 2012;19(7):857–8.
- Aziz MF, et al. Comparative effectiveness of the C-MAC video laryngoscope vs direct laryngoscopy. Anesthesiology. 2012;116(3):629–36.
- Lewis SR, et al. Video laryngoscopy vs direct laryngoscopy for adult tracheal intubation. Cochrane Database Syst Rev. 2016;(11): CD011136.
- Silverberg MJ, et al. Comparison of video and direct laryngoscopy in critically ill patients. Crit Care Med.2015;43(3):636–41.
- Turkstra TP, et al. Cervical spine motion: a comparison of video vs direct laryngoscopy. Anesthesiology. 2005;103(3):491–7.
- Doyle DJ. Videolaryngoscopy in the 21st century. Cleveland Clinic Journal of Medicine. 2021;88(5):263–4.
- Howard-Quijano K, et al. Video vs direct laryngoscopy teaching effectiveness. Anesth Analg. 2008;106(6):1651–4.
- Matava CT, et al. Safe Airway Management during COVID-19. Anesth Analg. 2020;131(1):61–73.
- Difficult Airway Society (DAS). Guidelines for the Management of Unanticipated Difficult Intubation in Adults. Br J Anaesth. 2015;115(6):827–48.
- American Society of Anesthesiologists (ASA). Practice Guidelines for Management of the Difficult Airway. Anesthesiology. 2022;136(1):31–81.
- Park L, et al. Use of handheld video laryngoscopes in the ICU. J Intensive Care Med. 2021;36(1):78–84.
- Sakles JC, et al. First-pass success rates with video vs direct laryngoscopy. Acad Emerg Med. 2013;20(7):617–23.
- Driver BE, et al. Optimizing Stylet Shaping for Hyperangulated Video Laryngoscopy. Ann Emerg Med. 2020;75(4):454–61.
- Yan Y, et al. Development of an AI system for airway structure identification in VL. J Biomed Inform. 2021;115:103704.
- Choi J, et al. Augmented reality in airway management training. J Clin Anesth. 2023;86:111086.
- Schricker T, et al. Disposable video laryngoscopes in austere environments. Can J Anesth. 2022;69(4):530–7.
- Kennedy CC, et al. Skill retention in direct laryngoscopy: a fading art? Chest. 2014;146(4):1189–95.
Develop Your Device IQ
VL-specific FAQs that apply to every VL device.
- VL is not just DL with a camera. Direct laryngoscopy is a line-of-sight technique; video laryngoscopy is not. VL brings the camera to the target, rather than bringing your eye to it. That single difference changes both how you see the airway and how you pass the tube, and treating it like direct laryngoscopy with a screen often leads to unnecessary difficulty or failure.
- A wide range of VL devices exists. Each has its own blade design, ergonomics, and image quality. They all send a camera image to a screen, but they do not behave the same. Know your specific device—how it boots, how long the battery lasts, how the screen displays, and how the optics perform in fog, glare, or secretions.
- Troubleshooting your device must be second nature. Fog, blood, secretions, and poor white balance can rapidly degrade your view. Every device has its own solutions—learn them before you are in trouble.
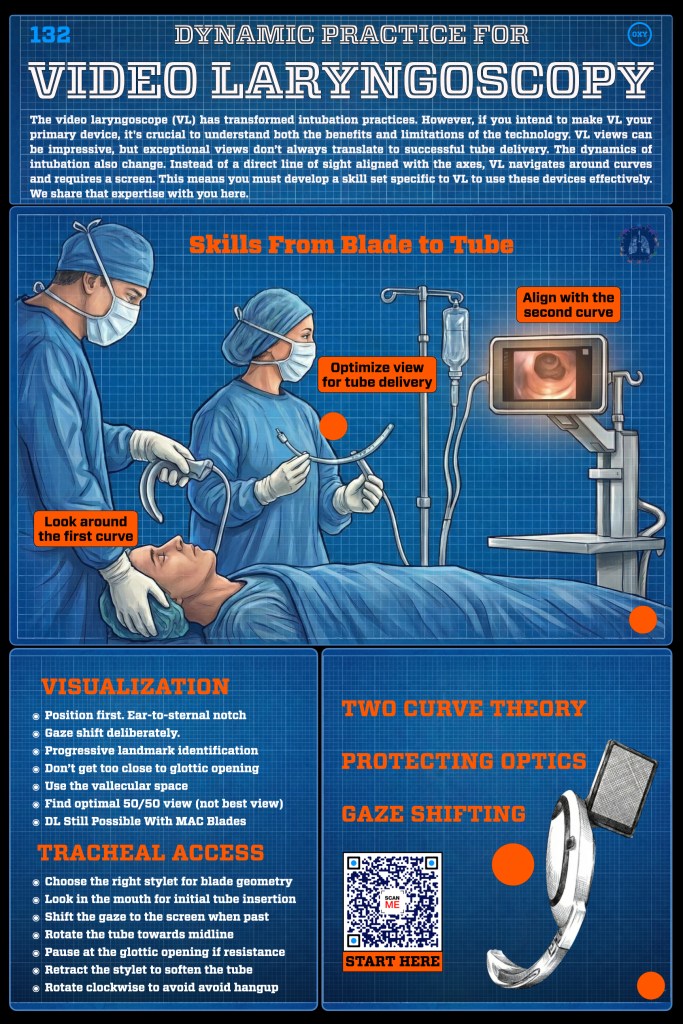
- Visualization & Tube Delivery Are Separate Problems. With VL, obtaining a clear view of the vocal cords does not guarantee successful intubation. The camera may provide an excellent glottic view, while the blade geometry and approach angle make tube passage more difficult. This mismatch commonly leads learners to fixate on the screen image and persist despite poor alignment for tube delivery. In VL, visualization is often easy, but optimizing that view for tube delivery is the defining skill, and failure to recognize this is a major source of difficulty.
- Blade selection matters. Macintosh‑style VL blades vary widely, and many cannot be used as traditional DL blades. Hyperangulated blades require a different technique and a rigidly shaped, pre‑formed tube.
- The Camera Is the Eye. Your visual reference point is the camera at the blade tip, not your eye. Small movements of the blade can produce large, sometimes disorienting changes on the screen. Successful VL use depends on maintaining orientation, protecting the camera, and resisting the urge to lift harder or to chase a better view when the image degrades.
- Tube Handling Is Different. VL requires intentional tube delivery skills. The endotracheal tube must be shaped to follow the curvature imposed by the blade, particularly when using hyperangulated blades. Advancing the tube too aggressively, too closely, or at the wrong angle commonly results in anterior hang-up or loss of orientation.
- Screen-Based Hand–Eye Coordination. VL changes where attention belongs and how movements are interpreted. Once the blade is inserted, visual focus must shift fully to the screen, while hands operate in a three-dimensional space guided by a two-dimensional image. This often feels awkward at first and can lead to overcorrection or exaggerated movements. Early discomfort is expected and should be anticipated rather than interpreted as failure.
- Battery readiness is essential. A dead or weak battery can compromise your entire plan, so confirm charge status and know how to manage backups.
- What Video Laryngoscopy Does (and Does Not) Solve. Video laryngoscopy reliably improves visualization and often increases first-pass success, but it does not solve all airway problems. It does not compensate for poor preparation, inadequate oxygenation strategies, massive contamination, or delayed decision-making. VL is a powerful tool for seeing the airway and for shared visualization during teaching and team-based care, but it does not replace sound judgment and experience. Understanding both its strengths and its limits is essential to using VL effectively and safely.
Dynamic Intubation Strategy
Roadmaps & Mental Models
A lot must happen before a laryngoscope is ever picked up. Successful intubation depends on clear cognitive frameworks that extend well beyond the mechanics of blade insertion. It requires deliberate planning and preparation at multiple levels, patient assessment, device selection, physiologic optimization, and coordinated individual and team readiness. The objective is not to “take a look.” It is to engineer first-pass success. An intubation attempt that is not optimized for first-pass success is, by definition, a wasted attempt.
Here, we’ll cover two of the most important cognitive frameworks that will improve your first pass success and, with it, patient safety.
Preparation & Planning (DAS25 Guidelines)
The DAS25 Guidelines
The VL Roadmap (The Two Curve Theory)
The Two Curve Theory
Dynamic Tracheal Access
Device Specifics
The video laryngoscope landscape is broad, with a wide range of devices and design differences. Before moving on, take a few minutes to become familiar with the specific device you use in your practice.
Click the links below to locate your device and review its key features.



Bottom Line

Video laryngoscopy didn’t just add a screen to a scope — it rewrote the rules. It shifted laryngoscopy from a solitary, analog task into a shared, digital process. As tools improve and training adapts, VL continues to evolve from a high-tech luxury to an essential skill for every airway provider. And in doing so, it’s not just helping us see better — it’s helping us think differently about the airway altogether.
What’s Next
Well done, you’ve completed this section.
To continue, visit the next poster in the series and scan the QR code. If you’re staying online, simply click the poster image here to move forward.
You must be logged in to post a comment.